YOU MAY WANT TO READ THIS IF:
- You work in healthcare in any capacity (e.g. nursing, physiotherapy, medicine, occupational therapy etc).
- You’ve considered (even vaguely) working away from the clinical setting for even a short while.
- You’re a friend or family member and I’ve begged you to read this.
HIT ME WITH YOUR BEST SHOT. I want to know how useful this post is. Would you be willing to comment below, or better yet, better yet, comment below AND book in a chat with me here?
If you’re reading this you’re probably the target audience, so your views are especially valuable to me.
SUMMARY
I’m technically a doctor but now working in a global health/public policy non-profit. I’m writing this because I was in search of a non-clinical experience as I approached the end of PGY2 in Australia. I disagree that you should wait to find non-clinical work, and there are many reasons I think you should crack on and try it out. Three that stood out for me are: it’s something I’m probably more interested in than 80% of my peers, a license to practice in healthcare is an incredible safety net, and, unless you want to be a rocket surgeon, you can probably afford to take some time away from the wards.
Hi – my name is Bal.
Technically I’m a doctor (AHPRA approved ✅), but right now I work in a non-clinical role as a program manager for a non-profit. My job has gone from putting in cannulas and writing discharge summaries to visiting paint factories and walking through spice markets (and writing lots and lots of emails – nothing is without its un-glamorous side).
The org I work for is called Lead Exposure Elimination Project (LEEP for short). We work with governments and paint manufacturers in LMICs to eliminate lead paint – 1/3 children around the world suffer from lead poisoning, a condition that has shockingly outsized effects on their health and on our global economy (5.5 million cardiovascular deaths each year and US $6 trillion lost globally (6.9% of global GDP).
I applied to work at LEEP because I was looking to try something outside of the hospital. I’d been interested in public and global health throughout medical school but never really engaged with it properly. As I started work in the hospital it felt like public health was getting further and further away, a distant goal separated from me by a growing mountain of discharge summaries to be done.
The role at LEEP was advertised as a chance to get stuck into public health and policy, see the world a little bit, and hopefully make some impact. So, I decided to dig my heels in and have a crack before I got caught up on a treadmill of clinical training — I reckon this was an incredibly low-risk gamble and I’ll get to why below.
It has been less than a year since I made that decision to leave the hospital for a bit of time, and as I approach the 12 month mark I thought it could be useful to reflect on the time gone by. This time last year I was on a mad search for help and advice and a whisper of opportunity to try something different, and a stray scrap of someone else’s story can sometimes make the dream seem a little more realistic.
I’m posting this because, at least amongst the medical professionals I asked, there was a little bit of hesitation at my idea of doing something non-clinical. The generic advice was to get some more clinical experience, build up some specialist expertise, and ‘smash out a training program’. (As if there is some way of speeding up time and accelerating the 6 years that most training programs require.)
I get it – you’re going to say that there isn’t much I can add to this topic, and I think you’re absolutely correct. This subject of clinical/non-clinical work is one that thousands of people have thought of before me and that people regularly write about. There’s an incredibly small chance that any of this is original, but as with a patient history, context is key. So, here are three reasons that motivated my decision to pursue non-clinical work:
- I’m probably more interested in doing something non-clinical than most of the people I studied with.
Ultimately, this reason boils down to interest/passion/desire for a certain topic. But to add some unnecessary complexity and diagrams, I think that one way to contextualise your interest in something is to say that there’s probably a normal distribution of interest (or disinterest) for any given specialty (e.g. paediatric physiotherapy, drug and alcohol medicine, ICU nursing). See my literal back-of-the-envelope diagram:
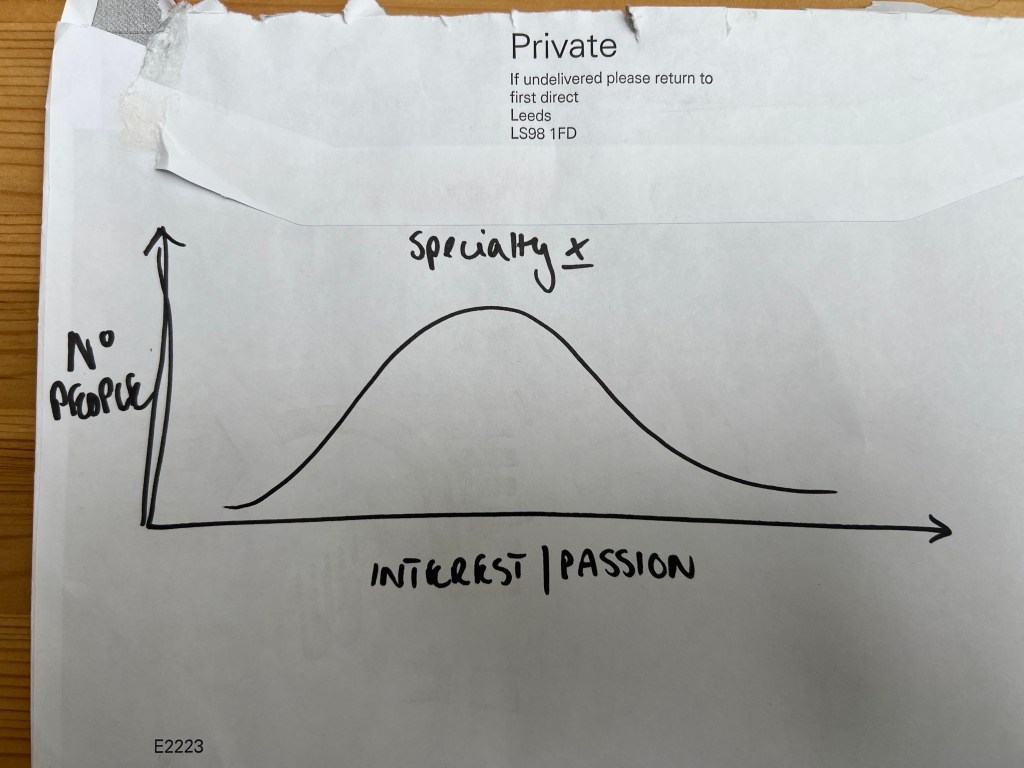
That’s not a particularly revolutionary idea, but I find it helpful as a reminder that the ideas that take up 80% of my career-thinking-time probably don’t take up that much time for everyone else. More than likely I share that with a smaller group of people.
I think that’s important to recognise because it’s probably some sort of predisposition. Put another way — I may have thoroughly enjoyed my orthopaedic term, but I don’t spend 80% of my career-thinking-time thinking about orthopaedic surgery. That puts me in-line with the larger proportion of people who have probably enjoyed their term and considered it as a career choice, but certainly behind the small percentage of people who are obsessed, which means it would probably be that much harder (on the margin and in expectation) for me to do as well as they will do.
That in and of itself is – truthfully – a totally fine outcome (i.e. aiming to be as good as the best orthopaedic surgeons is a pretty incredibly difficult goal). But I think it becomes a less palatable outcome when you think about wanting to have a particular, on-the-margin impact.
Put simply: even if I worked my arse off, I don’t think I’d be able to do as much for the world or the progression of orthopaedic surgery as my friends who grew up thinking about hammering bones every waking second since they could pick up a tool. By contrast, they probably spent less time thinking about public health issues like lead poisoning – so maybe that’s where I can find some marginal impact.
Accepting that logic, it becomes harder to justify not having a crack (so long as you are physically/mentally/financially able to).
- Getting a degree in a healthcare profession is going all-in on a sure bet.
“…in this world nothing can be said to be certain, except death and taxes (and the post-take ward round).”
Benjamin Franklin (mostly)
A degree in medicine, nursing, physiotherapy, or any other allied health is a ticket to security. Unless you have some other complicating factors (e.g. you’re an International Medical Graduate, you have restrictions on your license, you have geographical barriers etc), there’s next to no chance that there won’t be a job you can take. There is a global epidemic of healthcare shortages.
I get that it doesn’t feel right to encourage those shortages to become even shorter – someone somewhere is having chest pain, and someone somewhere else is one intervention away from a living life with significantly less disease – but the point to take from this is that (for most people), a degree in healthcare means enviable job security. And security means that you can make decisions that would otherwise seem risky.
It is surely why hundreds of medical graduates take time off every year to travel and locum. Like me, they’re also taking a step away from the standard structure of training (especially since locums don’t typically count towards training requirements), but have almost certain assurance that somewhere, sometime, there will be a ward round waiting for them when they return.
- You can move on a treamill, but treadmills themselves don’t move.
The big caveat to the reasons above is that you might be in the market for a hyper-competitive specialty. In that case, feel free to disregard/rebuke/criticise/openly slander this post.
If, however, your considered options for a clinical specialty aren’t gruellingly competitive, I’d suggest there’s a good chance you can take a year or two off work before getting stuck in to a training program. Next year, many of my friends will be taking up jobs as surgical registrars, GP trainees, or will start physician’s training. They’ve spent the past year studying, locum-ing, or just whiling away the time on a beach somewhere.
None of them seem to have been waylaid by a year of rest and recuperation. Some of them have even used the year to do something different, like overseas medical aid or management consulting. These experiences have given them something off the beaten track.
And when they get back to that hustling, bustling, overheated market of medical training, the treadmill training programs will still be in the same spot as they were a year or more ago. Sure, people will have clocked up a few kilometres in the meantime, but the treadmills aren’t currently going anywhere. And, for the most part, there’s almost always a spot free.
Some resources that helped me find non-clinical work:
- 80,000 Hours Job Board
- Job listings for orgs aligned with the Effective Altruism movement. The link takes you to jobs in Global Health & Development.
- High Impact Medicine
- A medicine-specific reading group aligned with the Effective Altruism movement.
- The group is an 8-week course of reading and discussion on areas in medicine (often non-clinical) that are ripe for making large impact.
HIT ME WITH YOUR BEST SHOT. I want to know how useful this post is. Would you be willing to comment below, or better yet, better yet, comment below AND book in a chat with me here?
If you’re reading this you’re probably the target audience, so your views are especially valuable to me.
